
LEAD is CMMI's correction, NOT its victory lap.
What the LEAD Model actually changes, what it preserves, and three scenarios for the next four years.


[Co-authored with Dr. Erin Hurlburt, Chief Medical Officer for Enablement at Lumeris]
From an operator’s perspective, LEAD feels less like a new chapter and more like a necessary course correction. For years, those of us on the front lines of value-based care have experienced a disconnect: we have been asked to take on the immense challenge of redesigning care for the frailest populations, yet the financial models often punish the very success we create. The PY2023 REACH evaluation laid this bare. CMMI validated what we were seeing: that even with genuine care improvements, a flawed benchmark could lead to ACOs experiencing unsustainable losses.
LEAD is their acknowledgment of this reality. It’s a signal that the goal isn’t just risk, but workable risk. CMMI is making this correction now because the data from both REACH and MSSP is undeniable. They are shifting the focus from simply testing a thesis to building a sustainable financial chassis that allows clinical innovation to thrive over the long-term, rather than drowning it in unforgiving math. This isn’t a victory lap for CMMI; it’s a pragmatic response to the evidence, and for that, it’s welcome.
We walked through the PY2023 evaluation and landed on an uncomfortable conclusion. REACH validated the high needs thesis dramatically, failed to validate the standard ACO thesis, and produced a financial methodology that made losses inevitable for roughly a quarter of participants. CMMI read the same data and responded in two ways. The first was a set of adjustments to REACH’s final performance year. The second was LEAD.
Understanding LEAD requires separating three things that tend to get collapsed in the trade press: What CMMI is changing on purpose, what CMMI is preserving on purpose, and what CMMI still does not know and is hoping a new model will teach them.
What CMMI is changing
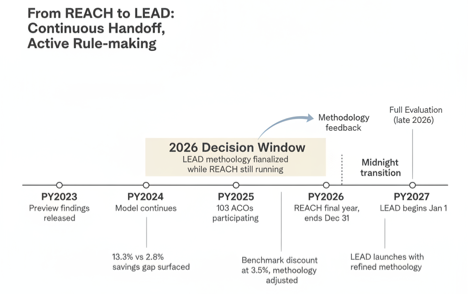
The most important change is financial methodology. The PY2023 evaluation surfaced a specific problem. The benchmark discount applied to REACH Global Option participants, 3% in PY2023 and PY2024 rising to 3.5% in PY2025 and PY2026, was large enough that organizations doing genuine care redesign could still end up in net loss positions simply because the math started against them. CMMI’s own PY2026 REACH adjustments and the framing of LEAD both point to a more nuanced benchmarking approach, one that attempts to distinguish between ACOs failing to manage care and ACOs succeeding at care management but drowning in benchmark mechanics. Whether LEAD actually solves this is an open question, but the intent is clear.
There is a second change nobody is talking about, which is the implicit narrowing of who LEAD is actually for. REACH’s standard track tried to be a big tent. The PY2023 data suggests that approach produced a wide performance distribution that masked what was actually working. LEAD’s design language, at least what has been released as of this writing, points to a narrower invitation. Organizations with genuine complex care management capability, existing capitation experience, and a multiyear commitment horizon. If that narrowing holds in the final rules, LEAD will be a smaller, more selective model than REACH. That is probably the right call on the merits and a political liability for CMMI simultaneously, because it means fewer participants, fewer jobs to announce, and a thinner constituency if the model comes under fire in 2028.
The third change is timing. LEAD starts January 1, 2027. There is no gap between models. That continuous handoff is not an accident. It forces CMMI to finalize LEAD’s methodology while REACH’s final year is still running, which means organizations will be operating under REACH rules through the end of 2026 while simultaneously evaluating and preparing for LEAD rules that are still being shaped. The next REACH evaluation is not expected until late 2026, which means LEAD will launch on rules that are partly informed by preliminary findings and will almost certainly be revised mid-model. Organizations should expect the LEAD rules they read in early 2026 to shift meaningfully before go live, and they should expect further revision after.
What CMMI is preserving
While the financial methodology is the headline change, some of the key components of REACH that CMMI is preserving in the transition to LEAD are just as telling, and the logic is fundamentally clinical. First, by retaining the provider-led governance requirements from REACH, CMMI reaffirms a critical lesson: clinical and financial decisions must be made by those who are directly accountable for achieving patient outcomes. This structure ensures that care design is guided by patient need, not just by a spreadsheet. It keeps the model grounded in the practical realities of care delivery.
Second, the continued commitment to full financial risk is the mechanism that truly empowers providers to break from the fee-for-service mindset. It’s what justifies the long-term investment in the interdisciplinary care teams, data analytics, and upstream interventions needed to manage complex populations effectively. The most innovative aspects of LEAD, like the CMS-Administered Risk Arrangements (CARA) and new capitation options, are only available to ACOs that select the Global, full-risk, track; this is by design. Without full risk, care transformation could remain just a pilot project; with it, it becomes the core business model.
Finally, carrying forward REACH’s benefit enhancements and adding novel incentives like the Substance Access BEI is a crucial nod to the realities of whole-person care. From a clinical perspective, these are not add-ons; they are essential tools that give care teams the flexibility to address the social and behavioral drivers of health that so often dictate outcomes. Additionally, CMMI views these flexibilities as a path to increase beneficiary interest in ACO participation rather than Medicare Advantage. Preserving these elements signals that CMMI understands that to succeed in value-based care, providers need more than just a new payment model; they need the right governance, the right incentives, and the right tools to do the job.
Three scenarios for the next four years
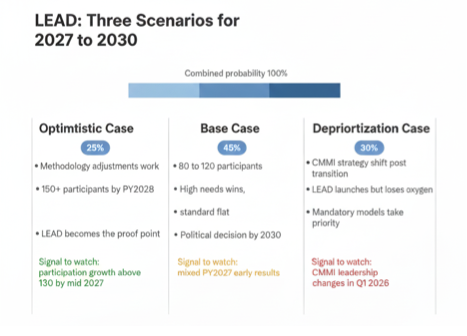
Scenario one, the optimistic case. CMMI’s PY2026 methodology adjustments work. The next REACH evaluation shows the PY2023 preview understated impact once later years are included. LEAD launches with a refined benchmark approach and attracts 150 plus participating entities by PY2028. High needs focused organizations continue to outperform, and a handful of standard track health systems crack the formula by running LEAD as a pure capitation chassis for their MA muscle. By 2030, CMMI points to LEAD as the model that proved full risk works at scale. Probability, roughly 25%.
Scenario two, the base case. LEAD launches on time, attracts 80 to 120 participants, and produces results that look a lot like REACH’s PY2023 evaluation. High needs organizations win. Standard organizations break even or lose modestly. Net Medicare FFS spending reductions remain elusive at the program level. CMMI spends PY2028 and PY2029 tweaking methodology. By 2030, the question of whether LEAD expands or expires becomes a political decision as much as an actuarial one. Probability, roughly 45%.
Scenario three, the one nobody is talking about but should be. A 2026 administration transition produces a CMMI leadership change that reorients accountable care strategy toward mandatory bundled payment models like TEAM and IOTA, direct Medicare Advantage expansion, and site neutral payment reform. LEAD launches on schedule in January 2027 because contracts are already in motion, but receives a fraction of the attention and investment CMMI originally planned. I think this scenario is underpriced in most health system strategic planning conversations I have been part of. The base case is still the base case, but scenario three is closer to 30% than the polite 20% most advisors are using, and it deserves explicit stress testing inside any LEAD investment decision. Probability, roughly 30%.
What this means for health system folks?
The complexity of your Medicare population is the single biggest predictor of whether LEAD economics will work for you. If you have a large frail, dual eligible, or multiple chronic condition cohort, LEAD is worth serious evaluation. If you do not, LEAD is probably not your model and MSSP remains the sensible path.
The 2026 decision window is not dead time. It is when LEAD’s economics are being decided while REACH’s final year is still being operated. Organizations engaging directly with CMMI, NAACOS, and APG during 2026 will have meaningfully more influence on final methodology than organizations that wait.
The political risk in scenario three is not zero and should not be ignored.
One question this series cannot answer and we would like smarter people to push back on. If LEAD’s financial methodology produces a more selective model that works well for high needs operators, does that advance CMMI’s 2030 goal of moving 100% of Medicare beneficiaries into an accountable care relationship, or does it quietly concede that full risk ACO models are a tool for a specific slice of the population rather than the main path? We have a view.
We are genuinely interested in whether people closer to CMMI policy think the goal and the model are still aligned, or whether LEAD is a signal the 2030 goal needs to be revisited.
 | A guest post by
|