The Map: How All 30 Models Layer Together
One Framework to Understand U.S. Healthcare Organization


You’ve now read about 30 distinct organizational models across 9 categories. If your head is spinning, that’s normal. American healthcare’s organizational complexity is not a bug — it’s the natural result of a system that evolved incrementally over 100 years, with each new model created to solve a specific problem without replacing the ones that came before.
Here’s how to think about it all.
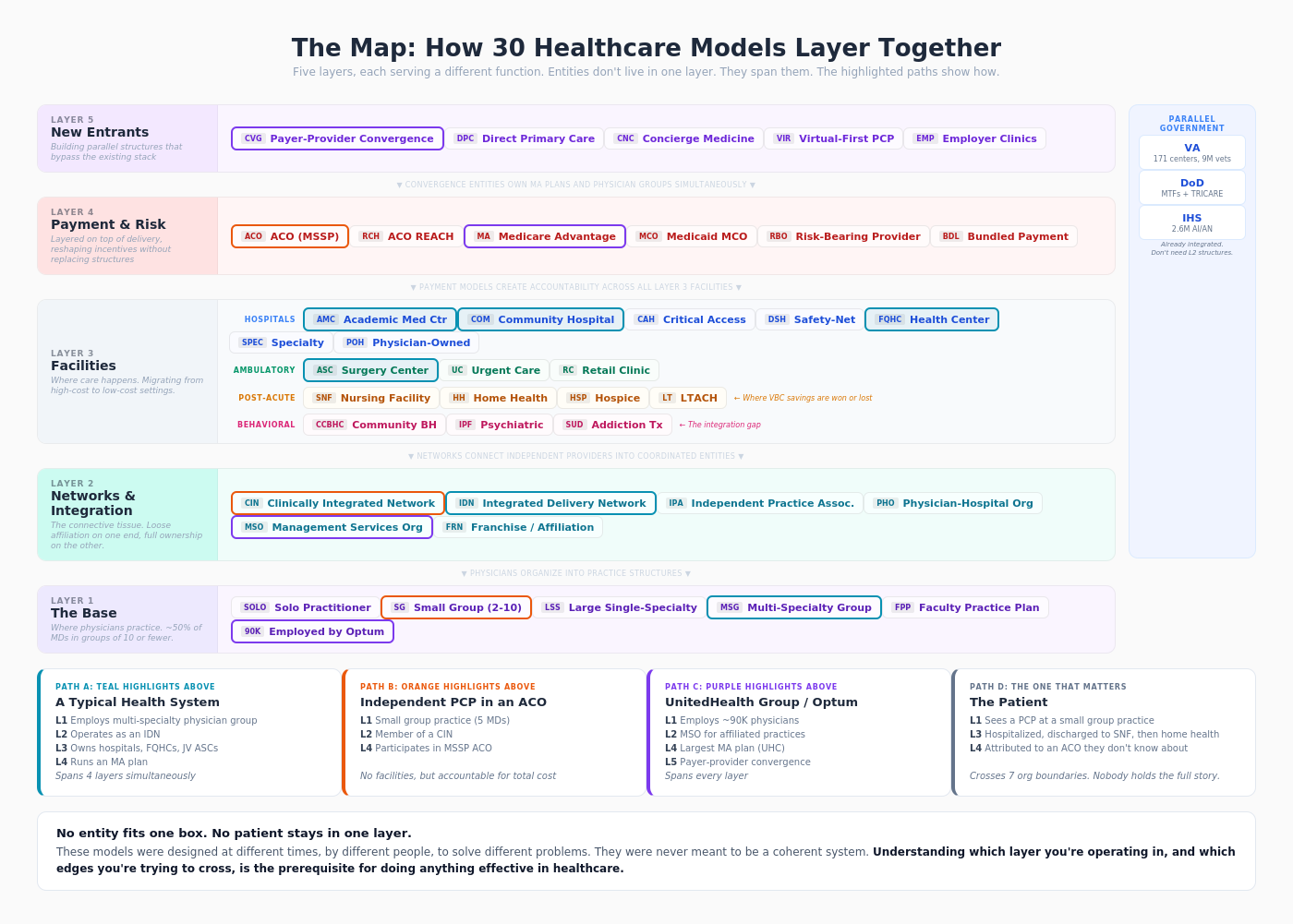
Layer 1: The Base — Where Physicians Practice
At the bottom are the practice models: solo practitioners, small groups, large single-specialty groups, multi-specialty groups, and faculty practice plans. This is where physicians actually see patients. Everything else is built on top of this layer.
Bottomline: About 50% of U.S. physicians still work in practices of 10 or fewer doctors. The base of American healthcare is smaller and more fragmented than most people realize.
Layer 2: The Connective Tissue — Networks and Integration
Above the practice layer sit the structures that connect independent providers into coordinated entities: CINs, IDNs, IPAs, PHOs, MSOs, and franchise/affiliation models. These exist because individual practices lack the scale, data, and infrastructure to participate in modern healthcare delivery and payment.
Bottomline: The spectrum from independence (IPA) to full integration (IDN) represents a fundamental tradeoff between autonomy and coordination. Most of American healthcare sits in the messy middle.
Layer 3: The Facilities — Where Care Happens
The physical infrastructure: AMCs, community hospitals, CAHs, safety-net hospitals, FQHCs, specialty hospitals, and physician-owned hospitals on the inpatient side. ASCs, urgent care clinics, and retail clinics on the outpatient side. SNFs, home health agencies, hospice organizations, and LTACHs on the post-acute side. CMHCs/CCBHCs, psychiatric facilities, and SUD treatment facilities for behavioral health.
Bottomline: Care is migrating from higher-cost to lower-cost settings — from hospital to ASC, from SNF to home health, from ER to urgent care. This migration is the dominant structural trend in healthcare delivery.
Layer 4: The Payment Models — Who Bears Risk
Layered on top of all the delivery infrastructure are the payment and risk structures: ACOs, ACO REACH, Medicare Advantage, Medicaid MCOs, risk-bearing provider organizations, and bundled payment programs. These don’t replace the delivery structures — they sit on top of them, reshaping incentives.
Bottomline: Payment models are the most powerful force reshaping healthcare organization. When you change how money flows, you change how care is delivered. Every organizational innovation in the past 15 years has been driven by the shift from fee-for-service to value-based care.
Layer 5: The New Entrants — Disrupting from Outside
Payer-provider convergence entities (Optum, CVS Health), DPC, concierge medicine, virtual-first primary care, and employer clinics represent models that route around the existing system’s limitations rather than working within them.
Bottomline: The most disruptive entrants are the vertical integrators — UnitedHealth/Optum, CVS/Aetna — who are assembling the full value chain under one corporate roof. They’re not playing within the existing structure. They’re building a parallel one.
The Government Parallel
Running alongside all of this are three massive government delivery systems — the VA, the Military Health System, and the Indian Health Service — that operate under completely different rules, funding mechanisms, and governance structures.
Why It Matters
The practical implication of all this complexity is that no single product, policy, or partnership strategy works across the entire healthcare system. A technology platform designed for an IDN won’t fit a solo practice. A payment model that works in California’s delegated market won’t work in a state where IPAs don’t exist. A care delivery innovation from an AMC won’t translate to a CAH.
Understanding which organizational model you’re dealing with — and which layer of the stack you’re operating in — is the prerequisite for doing anything effective in healthcare.
That’s the map. Use it well.