
Is CMS building the wrong half of the machine?

I know a someone who has been attributed to an ACO she has never heard of, by a doctor they see twice a year, for a condition they mostly manages through a spreadsheet their daughter updates on Sundays. The patient takes four medications, has opinions about three of them. Nobody at the ACO knows any of this, and nobody at the ACO is going to, because the ACO is not a place they goes. It is a piece of paper somewhere with their name on it.
This is what success looks like under the current CMS strategy. And I believe this is the fundamental problem.
I spend my days building products that sit inside this system. I watch smart teams pour themselves into programs that were never going to reach the people they were designed for, and I watch smart executives celebrate attribution numbers that would embarrass them if they ever had to explain what attribution actually means to their own mother. So when I look at the alphabet soup of CMS programs, at ACO REACH and APCM and MSSP and Making Care Primary and Primary Care First and now ACCESS and the just-announced LEAD model, I do not see chaos. I see a fifteen-year bet that was half-right and is about to run out of road.
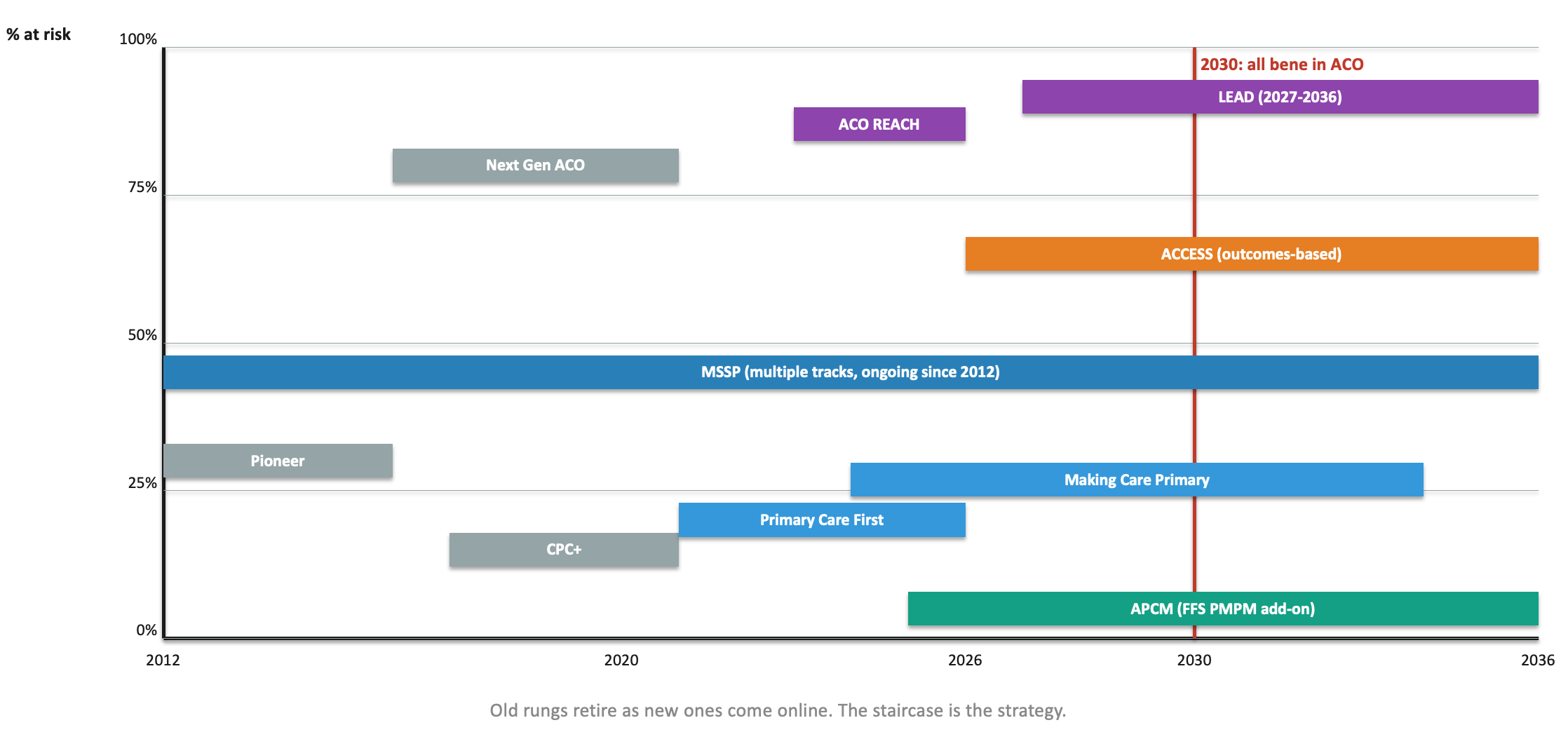
Fifteen years of rungs. All of them built for the supply side.
Here is the bet CMS made. If we pay provider organizations differently, beneficiaries will experience different care. Take more risk, build more infrastructure, coordinate more care, bill this new code. Every program in that staircase is one instruction repeated in a different dialect: provider, please change. It is a supply-side theory of everything. The goal, stated since 2021, is to have every Medicare beneficiary in an accountable care relationship by 2030. The machinery is aimed at getting providers into those relationships. The beneficiary is downstream of a formula.

The assumption under the whole thing is that if you get the supply side right, the demand side follows. And I am going to tell you, as someone who has spent years building for the supply side and who has skin in whether that assumption holds, that the assumption is starting to crack. ACO REACH will hit its participant targets and still leave most Medicare beneficiaries attributed through claims they never saw, to organizations they never chose, with care teams they never met. APCM will generate billions in new per-member-per-month revenue and most of it will fund existing staff doing existing work under a new code. MSSP’s savings curve has flattened. You cannot squeeze much more behavior change out of a system whose customers do not know they are in it.
The one program that breaks the pattern is ACCESS, the model CMS announced in December 2025. ACCESS is the first CMMI model that lets a beneficiary enroll directly, without an ACO wrapper, by walking into a digital front door. That is not a footnote. That is CMS quietly admitting the supply-side playbook has a ceiling and the only way through it is to let people opt into care models the way they opt into everything else in their lives. Once you see ACCESS that way, the rest of the portfolio starts to look like scaffolding for a building that has not been drawn yet.
Four versions of the future (aka…2032)
I think the honest way to talk about the next decade is to stop pretending there is one future and start drawing the four that are already happening in parallel
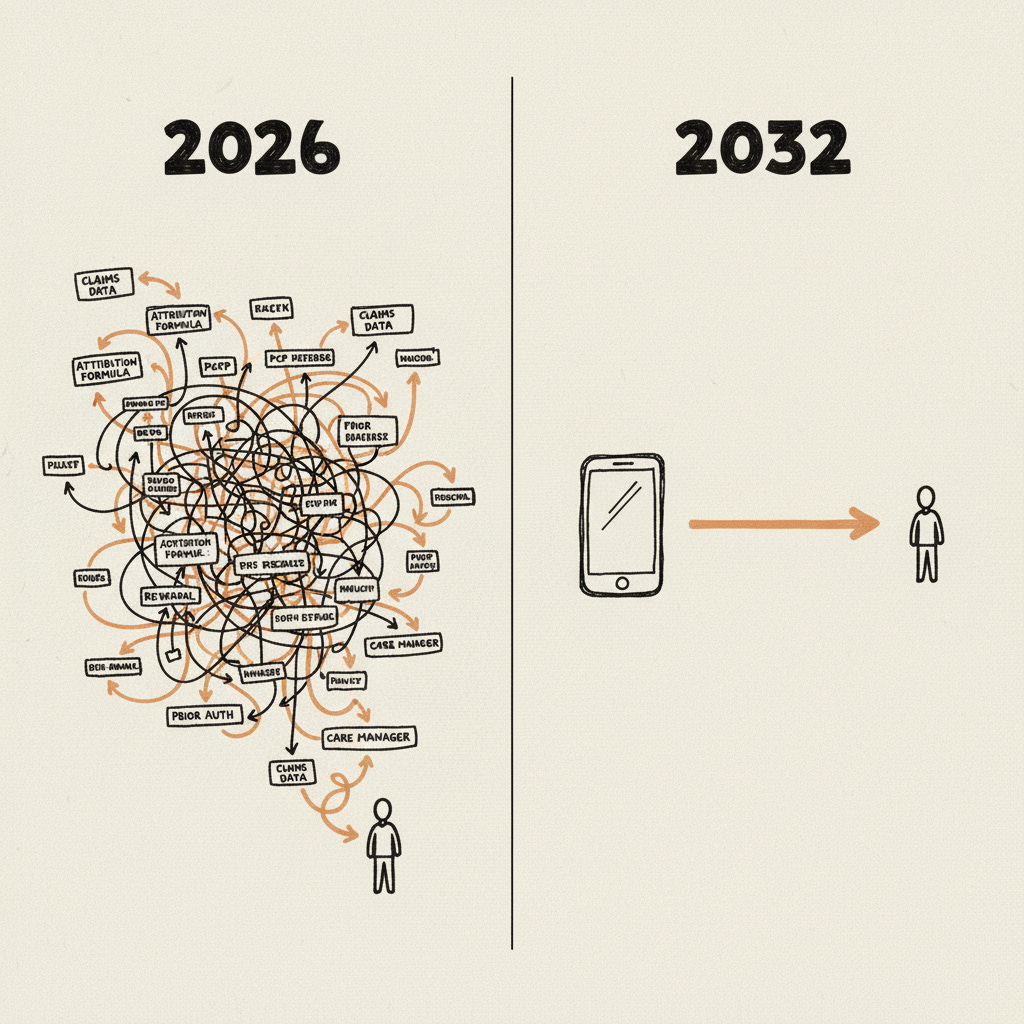
Left: how care starts today. Right: how it could start in 2032.
Future 1: The panel dissolves. By 2032, the patient panel is a legacy concept. Accountability is tracked per condition, per quarter, against outcome thresholds a beneficiary can see on their phone. A diabetic in rural Missouri has three condition-specific operators on her care team, none of whom are a primary care practice, all of whom get paid only if her A1c actually moves. The ACO still exists, but it is a back-office entity the way a PBM is. Necessary, invisible, increasingly commoditized. This is where the dual-eligible population goes first, because that is where the cost pressure is loudest and the political cover is thinnest.
Future 2: Beneficiaries choose. By 2032, Medicare beneficiaries pick their care model the way they pick a Medicare Advantage plan, except the choice is about outcomes, not networks. Enrollment happens on a phone, in ten minutes, with no provider referral. The organizations that win are the ones with the lowest cost per outcome improvement, regardless of whether they own a clinic. Attribution, the word that defined ACO policy for twenty years, has quietly disappeared from the vocabulary. This is urban Medicare Advantage racing ahead, the way banking did fifteen years ago when consumer choice finally showed up.
Future 3: AI collapses the cost curve. By 2032, the economics of intensive chronic care have flipped. What used to require a care manager and a nurse and a PCP and three handoffs runs on an AI concierge backed by a thin clinical layer. The downside risk that made outcomes-based models unbearable for operators has been absorbed by software. The winners are not health systems. They are operators who were software companies first and healthcare companies second. This is the thing underneath all the other futures, the reason any of them pencil.
Future 4: The CPT code eats the ACO. By 2032, commoditization is complete. Every care management capability that once required an ACO contract to fund is billable by any Part B provider as a standalone code. The ACO wrapper becomes a strategic choice, not a necessity. Some of the best outcomes in Medicare come from two-person practices in small towns running a stack of CPT codes and an AI layer, with no shared savings contract in sight. This is rural Medicare, held together by whoever is willing to drive the hour and whoever can bill the new codes.
These are not alternatives. They are happening at once, at different speeds, in different places, for different people. Rural goes to Future 4 because that is what rural can afford. Urban Medicare Advantage goes to Future 2 because that is where consumer choice has the oxygen to work. Dual-eligibles are the proving ground for Future 1 because cost pressure forces condition-level accountability there first. And Future 3 is the infrastructure layer underneath all three, silently deciding whether any of them pencil. The real question for the decade is not which future wins. It is which one arrives fastest and pulls the others along behind it.
Where I sit, and why I am telling you
I should stop and tell you something, because this piece is about to get more opinionated and you deserve to know whose opinion you are reading.
I am the VP of Product at Lumeris. When I look at those four futures, I am not a neutral observer. I have a bet, and it is on Future 3. The version of 2032 where AI collapses the cost curve of chronic care delivery enough that outcomes-based payment finally pencils for the operators who have to live inside it. That is the future I wake up trying to pull forward, and I believe in it.
And I want to be straight with you about something else. If I take off the operator hat and ask which of these futures is best for the person at the kitchen table with the pillbox, I do not think it is Future 3. I think it is Future 2. Choice is the only force that has ever meaningfully disciplined any part of American healthcare. Attribution is the opposite of choice. A system where tens of millions of people are assigned to care relationships they did not consent to, by formulas they cannot see, is not going to generate the outcomes we keep promising, no matter how elegant the risk-sharing math gets on the supply side.
So I am in a strange spot. I am building hardest for the future I think will win commercially. I am rooting loudest for a different future I think would be better for patients. And I am watching Futures 1 and 4 happen in the background for populations that neither my bet nor my hope is going to reach on time.
Here is why that is not actually a contradiction. Future 3 is the precondition for Future 2. You cannot offer people a meaningful choice between care models until the economics of those care models are good enough that operators can compete on outcomes instead of volume. Right now they cannot. The unit economics of intensive chronic care are so brutal that any operator who tries to compete on outcomes alone goes out of business before the second performance year. AI is the thing that changes that math, not because it replaces clinicians, but because it absorbs the coordination and documentation and follow-up and outreach costs that currently make outcomes-based contracts unbearable. Once that math flips, and I think we will know by about 2028 whether it has, the supply side is finally ready to be chosen from. That is when Future 2 becomes possible. Not before.
Future 1 and Future 4 are not detours from that path. They are the places where the new economics will prove themselves first, because they have to. Condition-level accountability will emerge in dual-eligibles because the old model is collapsing under cost. CPT-code-driven micro-practices will emerge in rural markets because the old model never really showed up there in the first place. Both will run ahead of the urban, technology-rich experiments everyone writes about, and both will teach Future 3 operators what actually works before Future 2 is ready to be built on top of it.
So the honest version of my bet is this. The boring half has to get built first, because the exciting half does not work without it. If the people doing that work do their jobs right, the best things they build will be invisible inside the care models patients eventually get to choose between. I am okay with that.
I would rather build the plumbing for the future I want to live in than write essays about it.
What has to be true
These are not policy recommendations. Neither you nor me are probably in the mood for another bullet list of everything Washington should do differently. These are the five things I am watching, because they are the ones that will tell me whether the bet I just described is working or quietly falling apart.
Direct enrollment has to spread beyond ACCESS. If the 2027 and 2028 CMMI models still route every beneficiary through attribution logic, the demand side never wakes up and Future 2 dies in the crib. ACCESS opened the door. Someone has to walk through it.
Outcomes thresholds have to be measured by someone the operator does not pay. The moment CMS lets ACCESS-style models grade their own homework, the model becomes a revenue scheme and nothing changes for the person at the kitchen table. This is the boring detail that decides whether any of it is real.
The cost curve has to actually bend, and it has to bend publicly. If AI-native operators cannot show, by 2028, that they are delivering measurably better chronic care at meaningfully lower cost than the status quo, Future 3 was a story and not a strategy. I will know where I stand by then. You will too.
At least one tech-native operator has to bill Medicare directly and win on outcomes, without a legacy provider laundering the services on their behalf. One existence proof is enough. Zero is not.
The primary care visit has to stop being the center of gravity. Not disappear. Just stop being the thing every care model is forced to route through. If 2032 still looks like a fifteen-minute office visit with AI duct-taped around the edges, we rebuilt the old system in new clothing and I will owe a lot of people an apology.
The close
None of this arrives cleanly. The pragmatic version of 2032 is that all four futures are happening at once, at different speeds, in different places, for different people. Rural Medicare looks like Future 4, held together by CPT codes and small practices and whoever is willing to drive the hour. Urban Medicare Advantage races into Future 2, where direct enrollment and consumer choice finally show up the way they showed up in banking fifteen years ago. Dual-eligibles become the proving ground for Future 1, condition-level accountability, because that is where the cost pressure is loudest. And Future 3 runs underneath all of it, quietly deciding whether any of this pencils at all.
CMS built the supply-side machinery with real skill and real patience, and it got further than a lot of people thought it would. But the bet it made, that fixing the provider side would pull the patient side along behind it, is the half of the machine that is running out of torque. The other half, the half where beneficiaries choose and operators compete on outcomes and AI makes the math work, is being built right now by a mix of policy accidents, tech-native operators, and infrastructure builders who are betting the next decade on it.
The organizations that win the next decade are the ones building for the future that is already arriving in pieces, not the one CMS keeps drawing on the whiteboard. I am betting my career on a specific one of those pieces. Now you know which, and why, and what I am watching for.